
Case study – Does regular exercise aid recovery from Guillain Barré Syndrome?
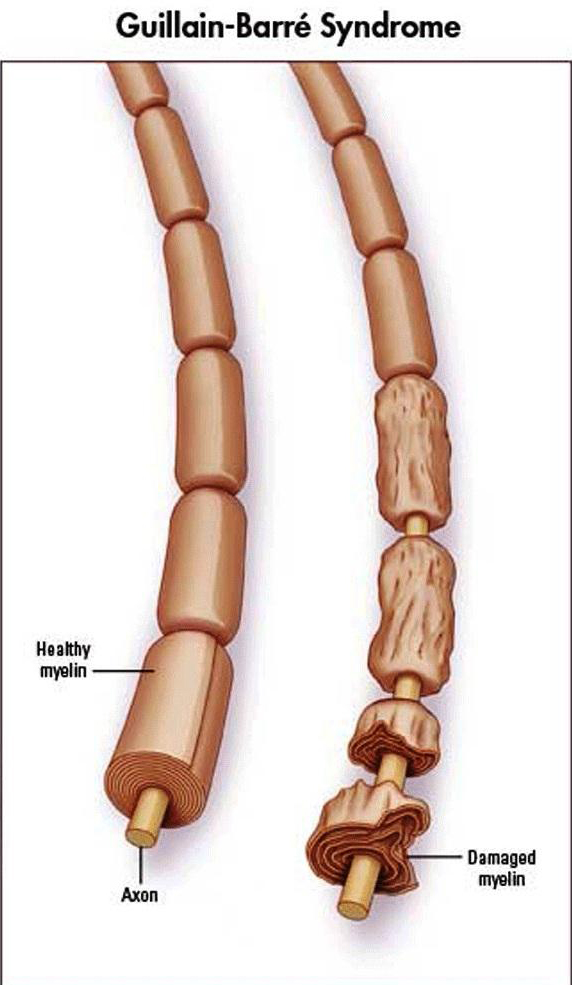
Guillain–Barré syndrome (GBS) is a neurological disorder which leads to a rapid onset of muscle weakness caused by the immune system damaging the peripheral nervous system. The first symptoms of GBS are numbness, tingling, and pain, either on their own or in combination. The weakness can take from half a day to over two weeks to reach maximum severity, and then becomes steady. The underlying mechanism involves an autoimmune disorder in which the body’s immune system mistakenly attacks the peripheral nerves and damages their myelin insulation, thus impairing nerve conduction
This is a recount of a person who I treated and trained. It highlights the benefits of training and rehabilitation exercises even a long time after a trauma had occurred.
“I contracted Guillain-Barré Syndrome (GBS), an autoimmune disorder affecting the peripheral nervous system, at the age of 50. The episode of GBS was moderate and had a fairly typical onset of ascending paralysis in both legs, partial paralysis/numbness in the arms, shoulders and hands but did not greatly affect the chest or breathing. I was able to walk with the aid of a stick within 6 weeks and started a phased return to work after 6 months. I was assessed by my neurology consultant as having achieved 80% recovery after 6 months, plateauing after 12 months at about 90% of my previous level of fitness. However, I continued to experience fatigue very easily and was left with some residual nerve damage down the right side of the body, with particular problems in the right leg due to muscle atrophy in the quadriceps muscles and poor neural motor control.
Initial NHS physiotherapist intervention was limited to providing a post-discharge self-directed home exercise programme to rebuild muscle strength and balance. Following some independent research, I decided to complement this with Pilates to help improve core stability, balance and thereby increase mobility. After self-referral for further physiotherapist assessment and treatment, continuing problems with poor gait, pain and muscle weakness were identified by the physiotherapist, who recommended a different programme of exercises and regular attendance at a gym. A subsequent MRI scan confirmed that there were no musculoskeletal problems, leading to the conclusion that the cause of the pain and weakness remained neurological.
I followed the various rehabilitation exercise programmes on a self-directed basis for a number of years, but the lack of knowledge and technique meant this began to have limited efficacy, eventually leading to a lack of motivation. I, therefore, engaged Antonino, an osteopath and personal trainer to help with technique and increase my repertoire of useful rehabilitation and general fitness exercises. This had a more successful outcome and greatly improved overall strength and mobility. Now aged 60, I continue with an exercise regime comprising one hour per week of supervised equipment-based Pilates plus one or two hourly gym sessions, one of which is usually with a personal trainer. Including supervised or 1:1 exercise sessions within the regime has proven to be more effective than self-directed exercise alone, where poor technique and loss of motivation became an issue. Fatigue, neural pain and muscle spasms remain a residual problem of the GBS, both during and after exercise sessions, and DOMS is possibly more acute than in a person without a similar neurological history, who would never experience ‘good’ pain. However, this has to be balanced by the fact that muscle strength and core stability are now greatly improved and, as a consequence, good mobility is maintained.
I am still training Mr J. At the moment, we are exploring whether end-range joint stretching flares up neurological pain in his right leg. In fact, Mr J has been following a supervised strength training which involves concentric gymnastic type body weight exercises and 75 – 80% 1RM free weight exercises. This training regime does not seem to trigger any side effects or neurological pain, although full range stretching and isometric training does trigger neurological pain in his right leg, especially in the right knee area. This is apparently due to a type of sensory nerve ending (type 1a or primary afferent fibres) getting overexcited during stretch proprioceptive movement, thus leading to a disorganised discharge of action potential along the nervous system that the brain interprets as pain. It is possible that stretching should not be taken at the end range and isometric exercises should not be performed extensively in training people with GBS.
